

Background
Eculizumab, a monoclonal antibody targeting C5, is an effective treatment for complement-mediated thrombotic microangiopathy (CM-TMA), also known as atypical hemolytic uremic syndrome. Although lifelong therapy has been suggested, the optimal treatment schedule is unknown, while eculizumab discontinuation does not universally lead to relapse. Data evaluating risk factors associated with an increased risk of CM-TMA recurrence following eculizumab withdrawal are scarce. Prior to the eculizumab era, complement genetic studies have been used to assess morbidity and mortality in patients with CM-TMA. Our aim was to assess the impact of complement gene variants on CM-TMA relapse rate (RR) after eculizumab discontinuation.
Methods
Search protocols were developed for the Ovid and PubMed databases to identify existing reports on CM-TMA and eculizumab withdrawal published before February 1st 2020. Cases were cross-referenced to eliminate duplicates. Inclusion criteria included patients diagnosed with CM-TMA who had undergone eculizumab discontinuation. Reasons for exclusion were patients with no follow-up after eculizumab withdrawal and patients lacking complement gene testing. Patients undergoing eculizumab dose extension, but not discontinuation, were not included.
Results
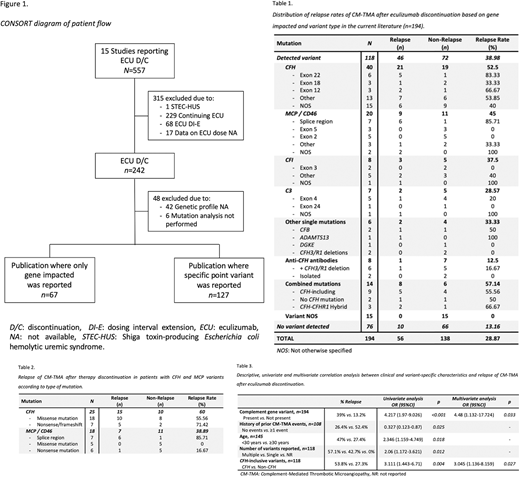
Fifteen studies including 557 individuals were retrieved. Of these, 363 (65.2%) were excluded as outlined in Figure 1 and 194 cases were included in the final analysis with a global RR of 28.9% (n=56). Distribution based on gene impacted and variant type are presented in Table 1. RR was highest among patients with CFH variants (52.5% to 60%) -particularly if involving exon 22 or nonsense mutations-, MCP/CD46 variants (38.9% to 45%) -particularly if affecting splice regions-, and cases with multiple concomitant variants (57.1%) -particularly those including CFH or a CFH-CFHR1 Hybrid (Table 2).
Patients with relapse were more likely to have the presence of a complement variant (p<0.001), history of previously resolved CM-TMA events (p=0.022), younger age (mean age 22.4 years for patients with relapse vs. 32.33 years for patients without relapse; p=0.002) and, within those with detected variants, multiple vs. single variants (p=0.002) and CFH-inclusive variants (p=0.003).
On univariate analysis, complement gene variants (OR 4.217 95%CI 1.97-9.026; p<0.001), age <30 years (OR 2.346 95%CI 1.159-4.749; p=0.018), and presence of multiple variants (OR 2.06 95%CI 1.172-3.621; p=0.012) or CFH-inclusive variants (OR 3.111 95%CI 1.443-6.71; p=0.004) were associated with increased odds of CM-TMA relapse, while no prior history of additional CM-TMA events was the only factor associated with lower RR (OR 0.327 95%CI 0.123-0.87; p=0.025). Presence of complement variants (OR 4.48 95%CI 1.132-17.724; p=0.033) and CFH-inclusive variants (OR 3.045 95%CI 1.136-8.159; p=0.027) were independently associated with increased RR on multivariate analysis (Table 3).
Conclusion
Relapse after eculizumab discontinuation is rare in cases with no genetic variants identified but can increase to more than 80% in high-risk subgroups. Complement genetic testing is not required for CM-TMA diagnosis or for initiation of complement inhibiting therapy; however, our results demonstrate the value of complement genetic testing when stratifying risk of patients for consideration of eculizumab discontinuation.
Sridharan:Alexion: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal